This page is designed to give you, your family and friends information about your upcoming heart surgery. It will explain what to expect before and after your operation. Please take the time to read this information. If there is anything you do not understand please talk to your health care team and ask them to explain.
Who are my healthcare team?
A variety of different professionals are in your health care team. Some you will see often, and some you may only see once or twice. Each member of the team provides specialised care and all members of the team are important to your recovery
- Cardiologist
- Cardiothoracic Surgeon
- Cardiothoracic Registrar (doctor who assists the surgeon)
- Anaesthetist
- Nurse
- Cardiothoracic Clinical Nurse Consultant (CNC)
- Physiotherapist
- Occupational Therapist
- Social Worker
- Pharmacist
Preparing for Your Heart Surgery Whilst in Hospital
What will happen before your operation?
- The Cardiothoracic Surgeon will visit you to discuss your operation.
- The Cardiothoracic Registrar will ask you to sign a consent form. It is very important that you know what you are consenting to and that you understand any associated risks. By signing the consent form you are giving permission for the surgery to happen and signing to say you understand the risk of the surgery. Before you sign the consent form, make sure you ask the doctor to answer any questions or concerns you have.
- You will need to have:
- a blood test
- a chest X-ray
- an ECG
- and any other tests that are requested by your Cardiothoracic Surgeon
- The Cardiothoracic CNC (nurse) will visit you to discuss your surgery and can answer any other questions you may have.
- The Physiotherapist will:
- Conduct an assessment including a simple test to see how well your lungs function (spirometry)
- Provide you with an exercise program
- It is very important to remove jewellery. This includes your wedding ring unless it cannot be removed (in this case it will be covered with tape). The reason it is best to remove your wedding ring is that sometimes the fingers can swell. If this were severe, the ring would have to be cut to remove it. Also, we cannot take responsibility for patient’s valuables. It is much safer to send valuables such as jewellery home with a trusted family member or friend.
- If you smoke, you MUST STOP. If you have smoked within 6 weeks of your operation, the risk of complications is much higher for people who smoke. Your surgeon may decide that these risks are too high to proceed with your operation. If you continue to smoke and don’t tell us, you are taking a serious risk with your health. Most people need help to quit, so talk with your health care team about alternative replacement therapy. You can decide the best therapy for you
Important Information for your Family and Friends
Can my family visit me before my operation?
Your family can visit you on the morning of your surgery. They can stay with you until you are transferred to the Operating Theatre. However, there will be some interruptions to allow you to be prepared for surgery.
Where should my family wait while I am in the Operating Theatre?
As it can take 5 hours or more until you arrive in the Intensive Care Unit (ICU), your relatives will probably be more comfortable waiting at home during this time. When the operation is finished, the doctor will phone your next of kin.
If your family chooses to wait at the hospital, they may wait in the ICU waiting room which is located on Level 2 of the Clinical Services Building. Use lift D to get there. Your family should notify the ICU reception staff that they are there so that one of the doctors can speak to them after your operation is finished.
When can my family visit me after my operation?
Visiting in the ICU is flexible. Your family may experience a wait upon their arrival to the ICU waiting room as a result of doctors’ rounds, tests and procedures. The ICU waiting room staff will let them know when they can see you.
During the first one or two days after your operation, you will need plenty of rest. Only close family members and friends will be able to visit you.
While you are in the ICU, only two visitors are allowed in at any one time.
Please organise for only one member of your family or friend to phone for information during your hospital stay. That one family member or friend should be the contact person for everyone else to get updates on your progress.
Flowers
ICU does not allow flowers. Please ask family and friends to wait until you have moved to the ward before bringing flowers.
The Evening before your Operation
- The Anaesthetist will visit you to make sure that you are fit for surgery.
- If you are fit for surgery the Anaesthetist will write a prescription for your premedication. Premedication can be a tablet or injection that is given the morning of your surgery to help you relax.
- Your nurse or the Anaesthetist should be able to tell you the estimated time of your operation.
- A ward orderly or nurse will use a surgical clipper to remove excess hair from your body, from your neck to your toes.
- You must remove any nail polish and makeup.
- You will need to have a shower using a special liquid antiseptic soap given to you by your nurse. You should not use any deodorants or apply any talcum powder after this shower.
- You will have your evening meal as usual.
- From midnight you will not be able to eat or drink anything. This to ensure that your stomach will be empty at the time of your operation.
The Morning of your Operation
- You will need to have another shower using antiseptic soap.
- After your shower, you will need to put on a hospital gown ready for the operating theatre.
- You will also be given a special “hat” to wear. If you are allergic to anything (not just medicines) your “hat” will be red. This is to remind the staff that you have an allergy.
- You may brush your teeth and rinse your mouth with water but you must not swallow the water.
- You will still be able to have your medications in the morning with a sip of water.
- Approximately 30 to 60 minutes before you go to the operating theatre you will be given your premedication which may make you feel drowsy.
- It is important to go to the toilet before you have your premedication because you must stay in bed once you have had it.
- Once you have been given your premedication we will put an oxygen mask on you to help you breathe.
- If you wear dentures or glasses you can wear them to the operating theatre if you wish. They will be removed once you are asleep and returned to you after your operation when you are transferred to the Intensive Care Unit (ICU).
- You will be taken to the operating theatre on a theatre trolley by a ward orderly and nurse.
Will my operation go ahead as planned?
In most cases, the operation will go ahead as planned, but unfortunately in some situations, it may need to be done later. Some of the reasons include:
- Another person may need emergency surgery and will need to take your place on the operating list.
- If there are no beds available in the ICU.
- If you develop an infection.
- If the doctor feels there is a need to improve or correct other medical problems first. This is to ensure that you are in the best possible condition before having heart surgery.
We acknowledge that this may be very stressful for you and your family. If this does happen, your operation will be rebooked as soon as possible. Sometimes, you will have your surgery with another Cardiothoracic Surgeon. This is because the referring surgeon may not be able to perform your surgery.
Your Operation
In this section, you will find a brief explanation of two of the most common types of heart surgery. These are;
- Coronary Artery Bypass Graft Surgery (CABG/bypass)
- Heart Valve Repair or Replacement Surgery
Coronary Artery Bypass Graft Surgery (CABG/bypass)
When the coronary arteries of your heart have blockages and blood is unable to flow easily to your heart, you may need to undergo coronary artery bypass graft surgery (CABG/bypass). CABG/bypass surgery involves using an artery and/or a vein (called a graft) to bypass these blockages. Bypassing the blockage improves the blood supply to your heart muscle. Grafts are from either:
- Arteries
- an artery from inside your chest (“internal mammary artery”)
- an artery from your arm (“radial artery”)
- Veins
- a vein from your leg
Your surgeon will decide which are the best blood vessels to use for you. Sometimes they may use a combination of both arteries and veins.
During CABG/bypass surgery, the surgeon will cut through your sternum/breastbone to reach your heart. Your heart will then be connected to a heart-lung machine. This machine will take over the function of your heart and lungs, permitting the surgeon to temporarily stop your heart. The surgeon then bypasses the blocked coronary arteries by grafting either a vein or artery. Your heart is then allowed to resume beating. It is disconnected from the heart-lung machine. At the end of the operation, the breastbone is pulled together tightly with stainless steel wires. These wires will stay in for the rest of your life and are unlikely to cause any problems. The breastbone can take up to 8 weeks to mend. The operation usually takes between 3 to 5 hours.
In some cases, the surgeon can perform this operation while your heart is still beating. This is called “off-pump” coronary artery bypass surgery.
You may have additional cuts depending on what blood vessels your surgeon uses to make the grafts. If they are only using an artery from your chest, you will not have any extra cuts. But if they are using a vein, you will have a long cut (or several smaller cuts) in your leg from where the vein is taken. If they are using an artery from your arm, you will also have a cut on your arm.
Heart Valve Repair or Replacement Surgery
We have four valves in our heart, two on each side. They act as one-way doors, helping the blood to flow in one direction. These valves can be damaged by infection or disease. They can also be faulty from birth. Damaged valves can obstruct normal blood flow in the heart and they may need to be repaired or replaced. If the valve needs to be replaced, there are different types of artificial valves available.
- Mechanical metal valves
- Tissue valves, made from a variety of sources.
Your surgeon will explain the strengths and weaknesses of each type of valve and help you choose the type that is best for you.
During valve replacement surgery your surgeon will cut through your sternum/breastbone to reach your heart. Your heart will then be connected to a heart-lung machine. This machine will take over the function of your heart and lungs, permitting the surgeon to temporarily stop your heart. The surgeon then replaces your heart valve. Your heart is then allowed to resume beating. It is disconnected from the heart-lung machine. At the end of the operation, the breastbone is pulled together tightly with stainless steel wires. These wires will stay in for the rest of your life and are unlikely to cause any problems. The breastbone can take up to 8 weeks to mend. Your surgeon will be able to estimate the length of time for your surgery.
Blood Transfusions
Many patients having heart surgery will need a blood transfusion. Some people worry about the risk of contracting a disease. In Australia, the risk of contracting a disease from a blood transfusion is extremely low.
If you have any concerns, you need to talk to one of your surgical team. Your nurse will be able to organise for one of the surgical team to see you. When you consent to have your heart surgery you will also be asked to consent to receive a blood transfusion.
After the Operation & The ICU
Once your operation is over you will be taken to the ICU.
The ICU is designed for the constant specialised care and monitoring that you need after your operation. Most people stay in ICU for 1 to 2 days before being transferred to the ward. Everyone is different, so you need to progress at your own pace and not be worried if you need to stay in the ICU a while longer.
The ICU can be very noisy. When you start to wake up, you may hear lots of different noises including machines that beep. Beeping machines don’t necessarily mean that there is a problem.
You may also be aware of several small tubes and other special equipment attached to your body. These will have been put there while you were having your operation. They will be removed as soon as it is safe to do so.
Breathing Tube (Endotracheal Tube (ET))
A plastic breathing tube (ET tube) will be placed in your mouth and down into your windpipe (trachea) while you are in the operating theatre. This will help you breathe until you are fully recovered from the effects of the anaesthetic.
The ET tube is connected to a machine called a “ventilator” which assists with your breathing.
The ET tube will be removed as soon as you are awake and strong enough to breathe on your own. This usually takes between six to ten hours after surgery. When the tube has been removed you will be given oxygen for a few days. This can be done through a facemask or small tubes (nasal prongs) that sit just inside your nose. It is normal for your voice to be a bit hoarse for a couple of days after the tube is removed and some patients complain of a “sore, scratchy throat”.
Once the ET tube is removed you will be able to suck on ice and have small sips of water.
On the day after your operation you will be able to have clear fluids and the following day you will be able to have a meal.
Oro-gastric Tube
An Oro-gastric tube is a thin plastic tube that is inserted through your mouth and into your stomach. This allows fluid to drain from your stomach to stop you from feeling sick. This tube and the breathing tube are usually removed at the same time.
Intravenous and Arterial Lines
After your operation you will have:
- Medications and fluids given through intravenous (IV) lines. These lines are usually taken out on the second day after your operation.
- An arterial line (in your wrist). The nurses will use this line to check your blood pressure. This also allows blood samples to be taken easily. It will be removed as soon as it is safe to do so.
Monitoring System
You will be connected to a monitoring system that allows the nurses to keep a close watch on your heart rate and rhythm, your temperature, blood pressure, and the oxygen levels in your blood. This information allows them to adjust treatments to assist your recovery.
Sometimes when you move around in bed, the monitor alarms may sound. This does not mean that there is anything wrong. The alarms are designed to alert the nurse to any change in the information collected by the monitor.
Pacing Wires
You may have fine wires (pacing wires) at the bottom of your chest wound. One end of these wires is sitting on your heart and the other end may be attached to a small box that is called a “temporary pacemaker.” This can be used to regulate your heartbeat if necessary. Not all patients will have these wires. Not all of those who have them will need to be attached to a temporary pacemaker.
The wires are usually taken out on the third or fourth day after your operation. This is a simple process that will be done by your nurse.
Urinary Catheter
A small tube called a “urinary catheter” will be put into your bladder during your operation to drain away urine. This means you do not have to use a bottle or a bedpan to pass urine. Sometimes this catheter gives people a sensation that makes them feel that they need to urinate. This sensation is normal. The catheter will usually be removed on the second day after your operation, or when you are able to walk to the toilet.
Chest Drains
After your operation, you will have two or three plastic drainage tubes coming from your chest. These tubes drain blood that builds up in your chest as a result of your operation.
Drainage from these tubes will gradually decrease. These tubes will usually be removed one or two days after your operation, either in the ICU or in the cardiothoracic ward.
Leg Drains
If a vein has been taken out from your leg during CABG/bypass surgery, small tubes will be inserted in the leg wounds to drain excess fluid from the wounds. These drains will be removed the day after your surgery.
Pain Relief
Regular pain medication is very important to ensure you are comfortable and are able to do your deep breathing and coughing exercises. These exercises are important for your recovery and will help prevent pneumonia and lung infections.
At first, you will be given pain relief medication continuously through your IV line/drip.
Once you are fully awake, you will be connected to a Patient Controlled Analgesia (PCA) machine. This machine allows you to get pain medication as you need it, by simply pressing a button. It means that you will be able to control your pain relief based on your pain level.
Once your breathing tube has been removed, you can also start taking tablets to help with your pain. Usually, you will be given a long-acting pain tablet. When you are taken off the PCA machine, if your pain is not relieved by the long-acting tablet, you can ask for extra pain tablets. This will be given every three to four hours depending on your pain.
Physiotherapy
Your physiotherapy will begin in the ICU once your breathing tube has been removed. The Physiotherapist will assess and provide you with individually tailored exercises. The exercises are aimed to improve your lung function and assist in your recovery.
Until you can do them on your own, nursing staff and physiotherapists will assist and teach you how to:
- get out of the bed
- sit out of the bed in a chair
- walk
- cough while supporting your wound
Elastic or Compression Stockings
During your hospital stay, you will need to wear elastic or compression stockings. The stockings help blood from your legs return to your heart and prevent fluid from building up in the legs. They also help to prevent blood clots.
The nurses will help you to put on and take off the stockings. Before you go home, the nurses in the ward will teach you and your carer how to do this.
The Cardiothoracic Ward (3 North)
Generally, you will be transferred to 3 North one to two days after your surgery. You will remain in this ward until you are either ready for discharge or transferred to another hospital.
The surgical team will visit you daily to monitor your progress. They will make adjustments to your treatment if required. Generally, we aim to get you home five days after your operation, although you may stay longer. This will depend on the type of operation you had and your progress afterward.
During this period it is important that you consider the following:
- If you are having difficulty with managing your personal care tasks such as showering and toileting in the hospital and are concerned about how you will complete these at home within your home environment, discuss this with the occupational therapist when they see you.
- If you live alone or if no one can stay with you for the first couple of weeks after you go home, let the nurses know. The nurses can ask a social worker to see you and arrange for possible services and help.
- If you have stairs at home, the physiotherapist will work with you to make sure you are able to use the stairs before you leave the hospital.
- If you have not opened your bowels by the third day after your operation, let the nurses know. They can organise a laxative for you. You will not be able to go home until the doctors are sure that your bowels are working properly.
- It is very important that you do not use your arms to help you get out of bed or out of your chair.
- It is important that you continue to walk around the ward as much as you can.
- When you are moving around in bed or in the chair, and when you cough, you must remember to support your chest.
- Your doctor will usually let you know the day before you are due to go home. This is to give you time to organise your transport home from hospital.
On the day you go home, you will be provided with discharge letters and prescriptions. You will also be given the contact details of your Cardiologist and Cardiothoracic Surgeon. This is for you to make your follow-up appointments.
Make sure you have the following things to take with you:
- A letter for your GP/local doctor, who you should see within two days and then again two weeks after your discharge. You may be required to see your GP/local doctor more often to follow up with any blood tests or medication changes.
- A letter for your Cardiologist, as you will need to make an appointment and see them four weeks after discharge.
- A letter for your Cardiothoracic Surgeon, as you will need to make an appointment and see them six weeks after discharge.
- A prescription for medications that you need to take after discharge.
- A copy of your discharge summary, which includes a list of the medications you need to take. Please make sure you understand when and why you are taking your medications before you leave the hospital.
- Two pairs of elastic stockings as you will need to wear them for six weeks after your surgery.
- Pain medication from the hospital pharmacy (if appropriate).
Transport home
- Pick up will either be from 3 North or
- Discharge lounge – ask staff for directions.
You must wear your seatbelt. A small pillow between the belt and your chest may help with any discomfort. You may sit up straight or rest semi-reclined in the car, whichever you find more comfortable.
You should not go home by public transport. Buses and trains can be very crowded and you need to avoid the “push and shove” that can happen.
If you have difficulty with transport home, please tell the staff as soon as possible.
Transfer of Care (discharge) Information Following Heart Surgery
Most patients have concerns after surgery. What can I expect? How should I care for my wounds? When can I go back to my normal activities? The following guidelines are intended to answer these questions. However, each person is unique, and you may have special needs or concerns. If you do not find an answer to your questions, ask your nurse or cardiothoracic surgeon for more information.
What to Expect After Heart Surgery
- Patients find that they get tired very easily, but most people feel back to normal within six to eight weeks after surgery.
- Soreness across your chest, neck, and back may persist for several months. Take prescribed pain medication to relieve discomfort.
- It is common to feel slightly breathless with activity.
- You can sleep on alternate sides, but you must not lay on your front.
- If you have an incision on your leg, it is normal to have swelling. Remember to elevate your affected leg while sitting.
- It is normal to have a decreased appetite. Eat small, frequent meals.
Care of your surgical wounds
If you have stitches, staples, and/or dressing, your GP/local doctor should remove them as directed by your surgical team.
After your dressing has been removed, gently wash the wounds with warm water and mild soap every day. Showers are okay. Lightly pat the wounds dry with a towel.
It is normal for your wound to be sore, a little numb or itchy, and to look slightly red or bruised. This will improve within several weeks.
If your wound becomes hot to touch, red, swollen, or begins to ooze, contact your GP/local doctor for advice as soon as possible.
Here are some ways you can help to lower your risk of getting an infection:
- Take special care to mobilise and get out of bed as soon as recommended by your health care team.
- Do not allow visitors to touch your wound/s and dressing.
- Always clean your hands either with an alcohol-based hand rub or soap and water before and after caring for your wound/s.
- Avoid using perfumes, soaps, creams, or powder on your wounds as these can irritate.
- If you are prescribed antibiotics, take the full course even if you feel better.
- Give up smoking.
- Monitor your blood sugar level if you have diabetes.
Medications
Your medications may have been changed while you were in hospital. You will be given a new list of all of your medications as part of your discharge summary.
It is important that you understand what your medications are for and when you need to take them. You need to follow your medication schedule and only take the medications on your list. If you are unsure you should check with your doctor or nurse before you leave hospital.
Do not take any other medications unless advised by your doctor.
If you are on Warfarin, your blood will need to be monitored by your GP/local doctor regularly.
Resuming Daily Activity and Exercise
Things you cannot do
- Do not lift or push more than 2 kilograms in the first 6 weeks
- Do not drive for 6 weeks after your surgery, until your surgeon gives you medical clearance
- For commercial driving, do not drive for 3 months after your surgery
- Sexual activity: wait for 3 to 4 weeks. Be well rested and chose a comfortable position that puts the least amount of stress on your chest
Daily activities you can do
Daily activities are the everyday tasks we need to do at home or work. When you return home it is important to maintain a balance between rest and activity.
Listen to your body and take it slowly.
- Walking is the best activity after heart surgery, feel free to walk outside.
- Pace yourself: light activity around the house, dressing, walking on level ground.
- Keep your activity at a level where you can carry on a conversation.
- If you are too short of breath, slow down.
Reduce or stop the activity
- If you feel pain, dizziness, difficulty breathing, palpitations, heavy sweating, tiredness
- If your heart is beating too fast
If symptoms recur, consult your GP/local doctor
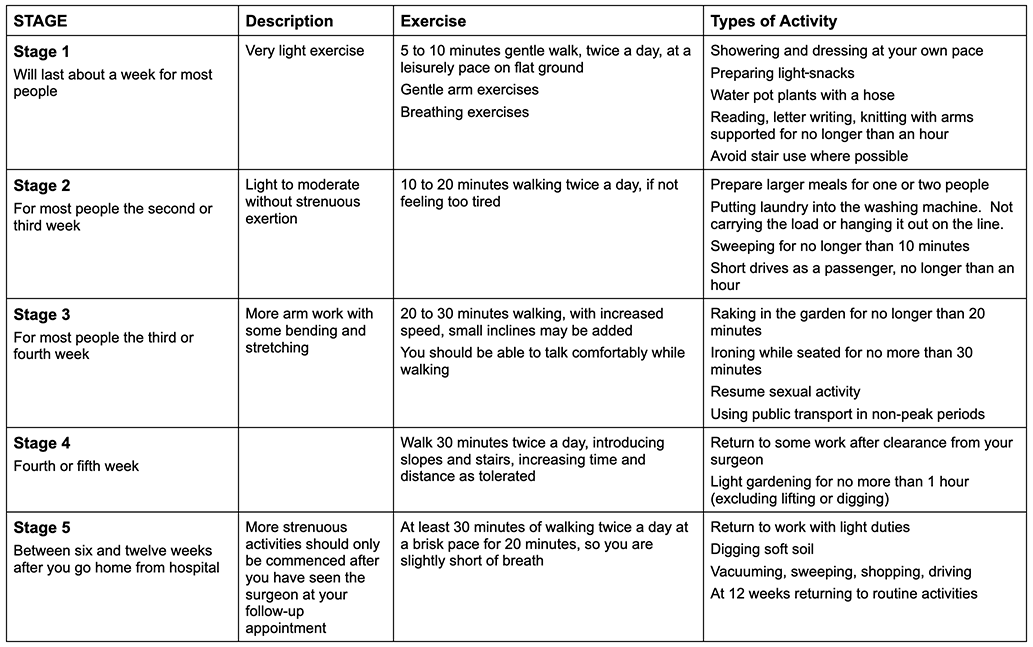
Exercise
A healthy lifestyle is important to help improve your physical fitness and maintain your wellbeing. A key part of this is ongoing regular exercise. Your exercises will be set for you by your health care team. As you recover, start thinking about lifelong exercises that you enjoy doing.
The next few pages will provide you an exercise guide you need to do at different stages of your recovery. Remember, this is only a guide, every person recovers at a different rate.
The following activities may be undertaken with care and at your own pace, as long as you are not lifting or pushing more than 2 kilograms in the first 6 weeks.
- Activities that involve excessive and prolonged arm movements, such as
- Washing the car
- Sawing wood
- Vacuum cleaning
- Painting
- Swimming
- Playing tennis or golf
- Activities that involve reaching above your head for prolonged periods, such as
- Hanging out washing
- Reaching into high cupboards
- Hanging curtains
- Pruning high bushes
- Pushing or pulling against objects that offer resistance, such as
- Mowing the lawn
- Unscrewing tight jar lids
- Moving furniture
- Exercising with weights
- Activities that involve bending from the hips and stooping
- Exercising less than 1 hour after eating or in extremes of temperature
Healthy Eating for Your Heart
Healthy eating can reduce the risk of problems that can contribute to your heart disease. This does not have to be boring or a ‘special diet’.
The following recommendations are some basic guidelines on healthy eating.
Healthy Eating Goals
- Enjoy a variety of foods from the main food groups. Eat vegetables, fruit, whole grains, lean protein and dairy every day. Make fresh foods the main part of your diet. Aim for 2 servings of fruit and 5 servings of vegetables daily.
- Consume 2 to 3 g plant sterols per day from margarine, breakfast cereals, reduced fat yoghurt or milk enriched with plant sterols.
- Watch out for unhealthy fats (saturated) these can contribute to unhealthy weight gain and increased cholesterol levels. Choose lean meat or trim the fat off meat and watch your serving size, try to keep to less than 350g red meat per week. Try to include 2 to 3 serves of fish weekly. Choose legume/bean-based meals during the week. Use reduced fat dairy products. Avoid the use of palm or coconut oils.
- Limit take away/deep fried foods like hamburgers, pizza, pies and chips.
- Limit snacks like doughnuts, cakes, biscuits, muffins, crisps.
- Choose healthier fats (polyunsaturated and monounsaturated) such as avocado, olives, nuts and seeds. Use olive, canola, sunflower and peanut oils (or spreads) in cooking.
- Choose healthy cooking methods. For example shallow frying, air frying, roasting, and casseroles instead of deep frying.
- Reduce salt. It is hidden in a lot of foods. Avoid adding salt to cooking or your plate. Use herbs and spices to flavour foods. Limit your intake of processed meats, take away foods, packaged foods and sauces. For sauces and packaged foods read the nutrition information panel and aim to keep sodium to less than 400mg per 100g or less than120mg per 100g is best.
- Make water your drink of choice. Avoid high energy drinks like soft drinks, cordials and juice. Limit alcohol to no more than 2 standard drinks a day (aim for 3 alcohol free days per week).
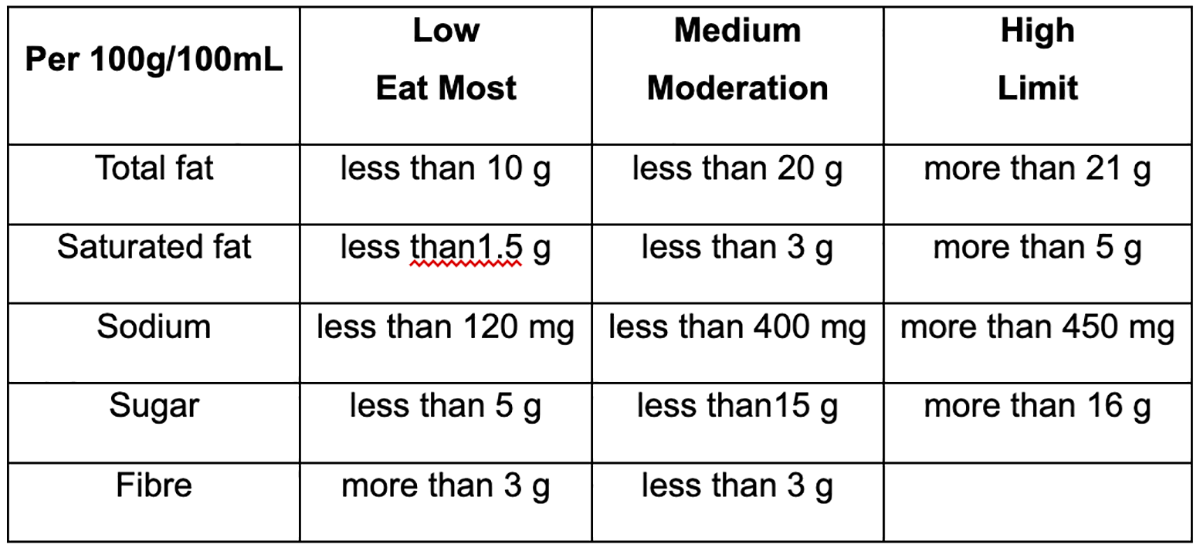
Shopping Guide
The nutrition information panels on various packaged foods (including sauces, snacks, cereals, etc) can give you an indication if this is the best choice for your heart health.
Remember
- Compare per 100g/100mL
- Ingredients list: limit if the first three are salt, sugar or fat
- Use the health star rating system for a guide to compare similar products together (aim for more than 3.5 stars)
- Dairy products and total fat: milk and yoghurt aim for less than 2g per100g and cheese aim for less than 15g per 100g
- Look for “salt reduced” or “no added salt” or “ low salt”
- Look for “low fat” or “fat free”
Useful contacts for additional healthy eating/nutrition information
- Cardiac rehabilitation program at your local hospital
- Get Healthy Service – free telephone coaching service https://www.gethealthynsw.com.au/, alternatively call 1300 806 258
- Referral from your GP/local doctor to an Accredited Practicing Dietitian. If you have a chronic disease (including type 2 diabetes) you may be eligible for a referral under Medicare.
- Heart Foundation https://www.heartfoundation.org.au
- Australian Dietary Guidelines https://www.eatforhealth.gov.au/
- Dietitians Australia https://dietitiansaustralia.org.au
Cardiac Rehabilitation – Cardiac Ambulatory Services
Following heart surgery, you are advised to attend cardiac rehabilitation, which is available at most hospitals. These programs are designed for patients discharged from hospital following treatment for a heart condition. This involves lifestyle education, exercise classes, and support. Cardiac rehabilitation programs have been proven to keep patients out of hospital and the patients tend to have better outcomes.
Cardiac Rehabilitation Programs:
Wollongong Hospital: 4253 4908
Figtree Hospital: 4255 5000
Bowral Hospital: 4861 0290
Further Information
Heart Foundation: https://www.heartfoundation.org.au/
When to Call for Help
If you have any of the following symptoms:
- Severe chest pain or tightness of chest
- Extreme shortness of breath
- Fainting
- Chest wound that begins to pull apart or starts leaking
- Fever greater than 38⁰ C and/or chills
- Palpitations or new onset of irregular heartbeats
- Dizziness or light-headedness that does not go away with rest
- Persistent nausea or vomiting
- Severe wound pain not relieved with pain medication
- Persistent fatigue
- Persistent depression
Who to Call for Help
In the event of an Emergency phone 000
If you are concerned or worried, please see your GP/local doctor
For advice, phone:
Cardiothoracic CNC (Mr David Sewell): 4286-1297 or phone Wollongong Private Hospital on 4286-1000 and ask for David Sewell.
Monday to Friday (excluding public holidays) 7:30am to 3:30pm
Cardiothoracic/Cardiology Ward 3 North: 4286-1255
Cardiothoracic Registrar: 4286 1000 and ask for the on-call Cardiothoracic Registrar.